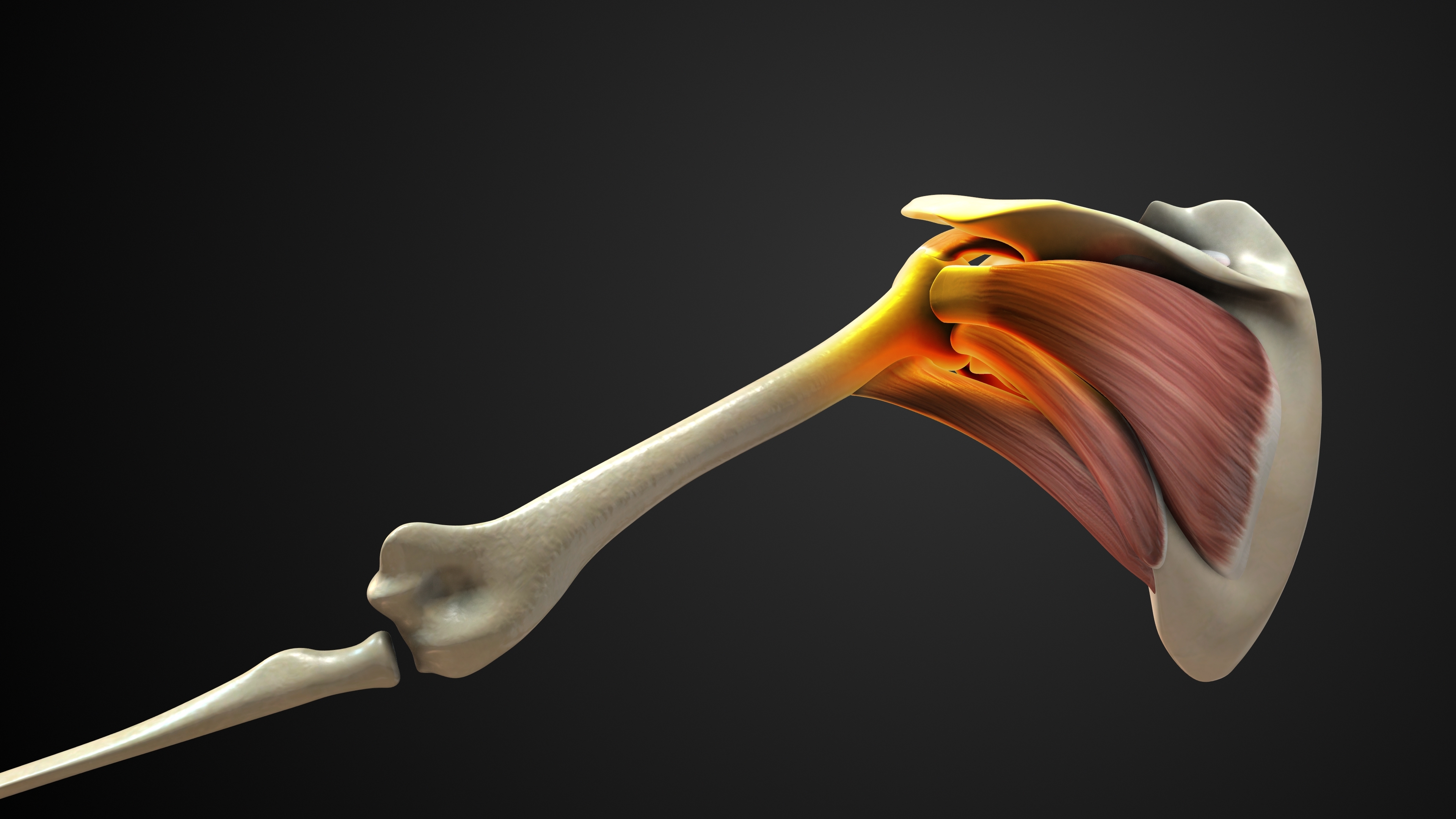
The rotator cuff is a group of four muscles and their associated tendons — the supraspinatus, infraspinatus, teres minor, and subscapularis — that collectively wrap around the head of the humerus, holding it firmly within the shallow glenoid socket of the shoulder blade. The rotator cuff is the essential dynamic stabiliser of the shoulder joint: it centres the humeral head during every movement of the arm, enables the full range of shoulder motion, and generates the force required for lifting, throwing, pushing, and pulling. Without a functioning rotator cuff, the shoulder cannot work normally.
A rotator cuff tear occurs when one or more of these tendons is partially or completely disrupted — either through a sudden traumatic event or through gradual degenerative wear over time. Rotator cuff tears are among the most common causes of shoulder pain and disability in adults, affecting athletes across all sports, active individuals, and older patients whose tendons have weakened with age. The supraspinatus tendon is the most commonly torn — accounting for the vast majority of rotator cuff injuries — due to its anatomical position under the acromion, where it is exposed to impingement with every overhead movement.
Dr. Konchwalla's extensive shoulder surgery expertise, FRCS qualifications from three Royal Colleges, and over two decades of specialist practice in Dubai make him the first choice for patients seeking definitive rotator cuff tear treatment. Whether your injury is a minor partial thickness tear amenable to physiotherapy, or a large full-thickness complete tear requiring arthroscopic repair with double-row suture anchor fixation, Dr. Konchwalla will design a precise, evidence-based treatment plan tailored to your specific tear, your age, your sport, and your recovery goals.